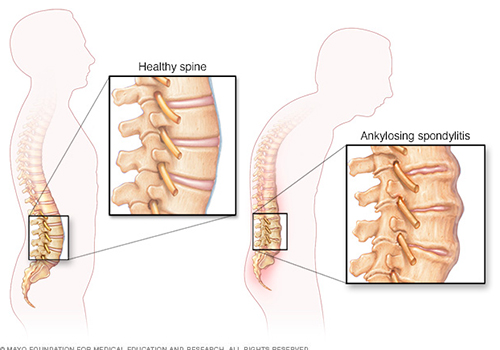
Ankylosing spondylitis (AS) is a type of arthritis that affects the spine.
It is a chronic condition in which the spinal joints and other joints of the body become inflamed. The symptoms include pain and stiffness from the neck down to the lower back. The spine’s bones (vertebrae) may grow or fuse together, resulting in a rigid spine. These changes may be mild or severe, and may lead to a stooped-over (bend down) posture. Early diagnosis and treatment helps control pain and stiffness and may reduce or prevent significant deformity.
There is no outright cure for ankylosing spondylitis, but there are treatments that can reduce discomfort and improve function. The goals of treatment are to reduce pain and stiffness, maintain a good posture, prevent deformity, and preserve the ability to perform normal activities. When properly treated, people with ankylosing spondylitis may lead fairly normal lives. Under ideal circumstances, a team approach to treat spondylitis is recommended. Members of the treatment team typically include the patient, doctor, physical therapist, and occupational therapist. In patients with severe deformities, surgery (osteotomy and fusion) can be done.
1. Physical and Occupational Therapy
Early treatment with physical and occupational therapy is the most important thing to maintain function and reduce the disability/ deformity.
2. Exercise
A program of daily exercise helps reduce stiffness, strengthen the muscles around the joints and prevent or reduce the risk of disability. Deep breathing exercises may help keep the chest cage flexible. Swimming is an excellent form of exercise for people with ankylosing spondylitis.
3. Medications
Certain drugs help provide relief from pain and stiffness, and allow patients to perform their exercises with minimal discomfort. Nonsteroidal anti-inflammatory drugs (NSAIDs) — such as ibuprofen, naproxen, and aspirin — are the most commonly used drugs for spondylitis treatment. In moderate to severe cases, other drugs may be added to the treatment regimen. Disease-modifying anitrheumatic drugs (DMARDs), such as methotrexate, can be used when NSAIDs alone are not enough to reduce the inflammation, stiffness, and pain. In addition, relatively new drugs called biologics — Cimzia (certolizumab pegol), Enbrel (etanercept), Humira (adalimumab), Remicade (infliximab), and Simponi (golimumab) — have been FDA-approved for treating ankylosing spondylitis.
Steroid injections into the joint or tendon may be helpful in some cases.
4. Surgery
Artificial joint replacement surgery may be a treatment option for some people with advanced joint disease affecting the hips or knees.
In addition, people with spondylitis are urged to not smoke or chew tobacco products because smoking aggravates the condition. Certainly, all of the other reasons why doctors discourage smoking also apply here as well.
People with spondylitis are encouraged to sleep on a firm mattress with the back straight. Placing large pillows under the head is discouraged, since it may promote neck fusion in the bend position. Similarly, keeping the legs up on pillows should be avoided because it may lead to hip or knee fusion in the bent position. Choose chairs, tables, and other work surfaces that will help avoid slumping or stooping. Armchairs are preferred over chairs without arms.
Since those with ankylosing spondylitis could easily hurt their rigid necks or backs, special care should be taken to avoid sudden impact, such as jumping or falling.
Special Precautions
A patient of ankylosing spondylitis who has developed a stiff spine with stooped (bent forward) posture needs to be aware of special precautions he/she has to take as well as inform the treating doctor, if such a patient happens to suffer from any spinal injury/fracture. The usual tendency after spinal injury is to make the patient lie straight on a hard board, but patients with ankylosing spondylitis should make it clear that they should be positioned in whatever posture they had developed prior to the injury because any forceful attempt to make them lie absolutely straight can cause grave damage to the spinal cord and risk causing paralysis.
Although the cause of ankylosing spondylitis is unknown, there is a strong genetic or family link. Most, but not all, people with spondylitis carry a gene called HLA-B27. Although people carrying this gene are more likely to develop spondylitis, it is also found in up to 10% of people who have no signs of the condition.
1. Pain and Stiffness
Constant pain and stiffness in the low back and hips that continue for more than three months. Spondylitis often starts around the sacroiliac joints (joint of the pelvis), where the sacrum (the lowest major part of the spine) joins the ilium bone of the pelvis in the lower back region.
2. Bony Fusion
Ankylosing spondylitis can cause an overgrowth of the bones, which may lead to abnormal joining of bones, called “bony fusion.” Fusion affecting bones of the neck, back, or hips may impair a person’s flexibility and ability to perform routine activities. Fusion of the ribs to the spine or breastbone may limit a person’s ability to expand his or her chest when taking a deep breath and cause breathlessness.
3. Pain In Ligaments And Tendons
Spondylitis also may affect some of the ligaments (structure which connect bone to bone) and tendons (structure which connect muscle to bone) that attach to bones. Tendonitis (inflammation of the tendon) may cause pain and stiffness in the area behind or beneath the heel or at the back of the ankle.
Other Symptoms :
1. Back Pain
The main symptom is back pain. The pain usually starts in the lower back. It becomes gradually worse over several months. The pain may be present over the hips, and down the back of thighs. The buttock pain may be felt sometimes on one side and sometimes on the other side. Coughing or straining may make increase the pain. Rest does not make it better. In fact, the pain may wake one from sleep. Instead, exercise and movement usually ease the pain. (This is the opposite to the bouts of common mechanical backache which may alert a doctor to the diagnosis of AS.) The pain tends to be worse first thing in the morning. Lying in bed after waking is often uncomfortable. The pain tends to ease as the day goes on.
The middle (chest part) of the spine may become affected. If this occurs, the joints between the ribs and the spine may also become painful.
2. Stiffness In The Lower Spine
The stiffness can be quite severe first thing each morning. It usually improves with activity and exercise, and tends to ease as the day goes on.
3. Other Joint Symptoms Apart From The Spine
Other joints are affected at some stage in about 4 out of 10 cases. The most common are the hips, knees, ankles, and shoulders. Affected joints can become painful, stiff, and swollen.
4. Inflammation Of Tendons And Ligaments
Tendons and ligaments in various parts of the body (in addition to those attached to the bones (vertebrae) of the lower spine) may become inflamed and painful where they attach to bones. Common examples are the Achilles tendon where it attaches to the heel, and where chest muscles attach to the ribs.
5. Inflammation Of Part Of The Eye (Uveitis)
Have AS and develop a painful or red eye. If you develop uveitis, treatment with eye drops should be started as soon as possible after eye symptoms begin. Treatment of uveitis is usually successful. However, if not treated quickly there can be permanent loss of vision in the eye (partial or complete).
6. General Symptoms
Some people with AS feel generally unwell with symptoms of tiredness or depression. Weight loss or anaemia can also occur.
A diagnosis of ankylosing spondylitis is based largely on the findings of a medical history and physical exam. Radiologic tests (X-ray or MRI) and lab tests may be used to help confirm a diagnosis, but both have some limitations.
Medical History :
The medical history involves answering questions, such as the following:
- How long have you had pain?
- Where specifically is the pain in your back or neck? Are other joints affected?
- Is back pain better with exercise and worse after inactivity, such as when you first get up in the morning?
- Do you have other problems, such as eye problems or fatigue?
- Does anyone in your family have back problems or arthritis?
- Have you recently suffered from a gastric trouble?
- Do you have any skin redness or rashes?
Physical Examination :
During the physical examination, the doctor will look for signs and symptoms that are consistent with ankylosing spondylitis. These include pain along the spine and/or in the pelvis, hip joints, heels, and chest. The doctor may ask you to move and bend in different directions to check the flexibility of your spine and to breathe deeply to check for any problems with chest expansion, which could be caused by inflammation in the joints where the ribs attach to the spine.
Radiologic Tests :
X ray and magnetic resonance imaging (MRI) may be used in making or confirming a diagnosis of ankylosing spondylitis, but these tests have limitations. X rays may show changes in the spine and sacroiliac joints that indicate ankylosing spondylitis; however, it may take years of inflammation to cause damage that is visible on x rays. MRI may allow for earlier diagnosis, because it can show damage to soft tissues and bone before it can be seen on an x ray.
Lab Tests :
The main blood test for ankylosing spondylitis is to check for the HLA-B27 gene, which is present in the majority of Caucasians with ankylosing spondylitis. However, this test also has some limitations. The gene is found in much lower percentages of African Americans with ankylosing spondylitis and in ankylosing spondylitis patients from some Mediterranean countries. Also, the gene is found in some people who do not have ankylosing spondylitis, and will never get it. Still, when the gene is found in people who have symptoms of ankylosing spondylitis and/or x-ray evidence of ankylosing spondylitis, this finding helps support the ankylosing spondylitis diagnosis.