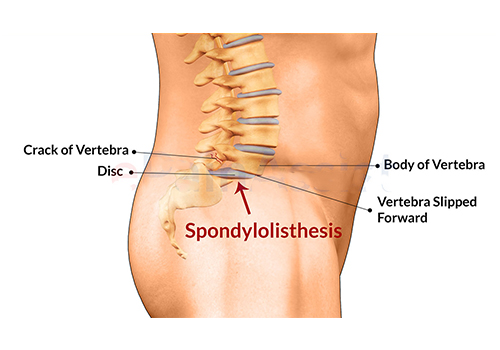
Spondylolisthesis is the abnormal forward displacement of a vertebra, especially the fifth lumbar vertebra, most commonly occurring after a break or fracture. Backward displacement is referred to as retrolisthesis.
Our spinal column consists of multiple small bones (vertebrae) perfectly stacked one over each other. Sometimes, one bone in the back (vertebra) slides forward over the next bone below it, thus disturbing the harmonious arrangement. It most often occurs in the lower spine (lumbosacral area). In some cases, this may lead to the spinal cord or nerve roots getting squeezed or stretched. This can cause back pain and numbness or weakness in one or both legs. In rare cases, it can also lead to losing control over your bladder or bowels.
occasionally, one may not have much symptoms despite having a slipped vertebra in his/her back. Then, pain in the low back or buttock occurs after sometime. Muscles in the leg may feel tight or weak. One may even limp also.
Spondylolisthesis is categorized into five types :
Isthmic spondylolisthesis
Isthmic spondylolisthesis is the most common form; also called spondylolytic spondylolisthesis. A slip or fracture of the intravertebral joint is usually acquired between the ages of 6 and 16 years, but remains unnoticed until adulthood. Roughly 90 percent of these isthmic slips are low-grade minimal slip (less than 50 percent slip) and 10 percent are high-grade major slip (greater than 50 percent slip).
Degenerative spondylolisthesis
Degenerative spondylolisthesis is a disease of the older adult that develops as a result of arthritis and joint remodeling in the back that in combination with ligamentum flavum weakness, may result in slippage of a vertebra. Degenerative forms are more likely to occur in women.
Dysplastic spondylolisthesis
Dysplastic spondylolisthesis is a rare congenital (present by birth) spondylolisthesis occurring because of a malformation of the lumbosacral junction, resulting in small, incompetent facet joints.
Symptoms of Spondylolisthesis Include
- A general stiffening of the back and a tightening of the hamstrings (muscles at the back of thighs), with a resulting change in both posture and gait.
- A leaning-forward or semiposture may be seen, due to compensatory changes.
- A “waddle” may be seen in more advanced cases, due to compensatory rotation of pelvis.
- A result of the change in gait is often a noticeable atrophy in the gluteal muscles (muscles of the buttocks) due to lack of use.
- Generalized lower-back pain may also be seen, with intermittent shooting pain from the buttocks to the back of thigh, and/or lower leg via thesciatic nerve.
- Some patients may experience difficulty in walking beyond a few minutes, when they develop pain and numbness in the thighs and legs
Conservative Treatment
Patients with symptomatic spondylolisthesis are initially offered conservative treatment consisting of activity modification, medical management and a physical therapy rehabilitation program.
Physical therapy can evaluate and address postural and compensatory movement abnormalities.
Anti-inflammatory medications (NSAIDS or pain killers) can be tried initially. If a severe radicular leg pain is present, some doctors may prescribe a short course of steroid medication given as tablets. Epidural steroid injections, performed under x-ray guidance can help reduce the severe radicular (leg) pain. Lumbosacral belt may be of benefit for some patients but should be used on a temporary basis to prevent spinal muscle weakness.
Surgical Treatment
Degenerative spondylolisthesis with spinal stenosis is one of the most common indications for spine surgery among older adults.
A spinal fusion for spondylolisthesis is generally quite effective, but because it is a large surgery with a long recovery time, it usually is not considered until a patient has failed six months of concerted non-surgical treatment.
Isthmic spondylolisthesis above the L5-S1 level (L4-5 or L3-4) is more likely to need surgery because of the amount of motion in the upper vertebral segments. It is less likely that a spondylolisthesis at L5-S1 will need surgery. However, because the incidence of spondylolisthesis is so much higher at L5-S1, most surgeries will still be at L5-S1 due to unremitting symptoms.
The L5-S1 segment at the bottom of the spine is not a major motion segment as it is deep in the pelvis, and it is also not really designed to move much. This is an important point because if this level is fused, it does not transfer a lot of stress to the other levels of the spine.
After an L5-S1 fusion, the spine is still biomechanically much the same as it was preoperatively, and most patients will not perceive any difference in their motion after a one-level lumbar fusion.